
How To A Radiology Assistant Radio Choices
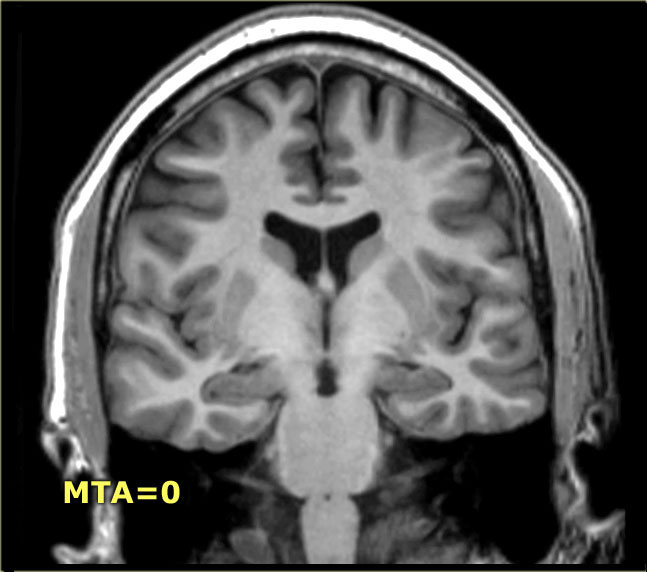
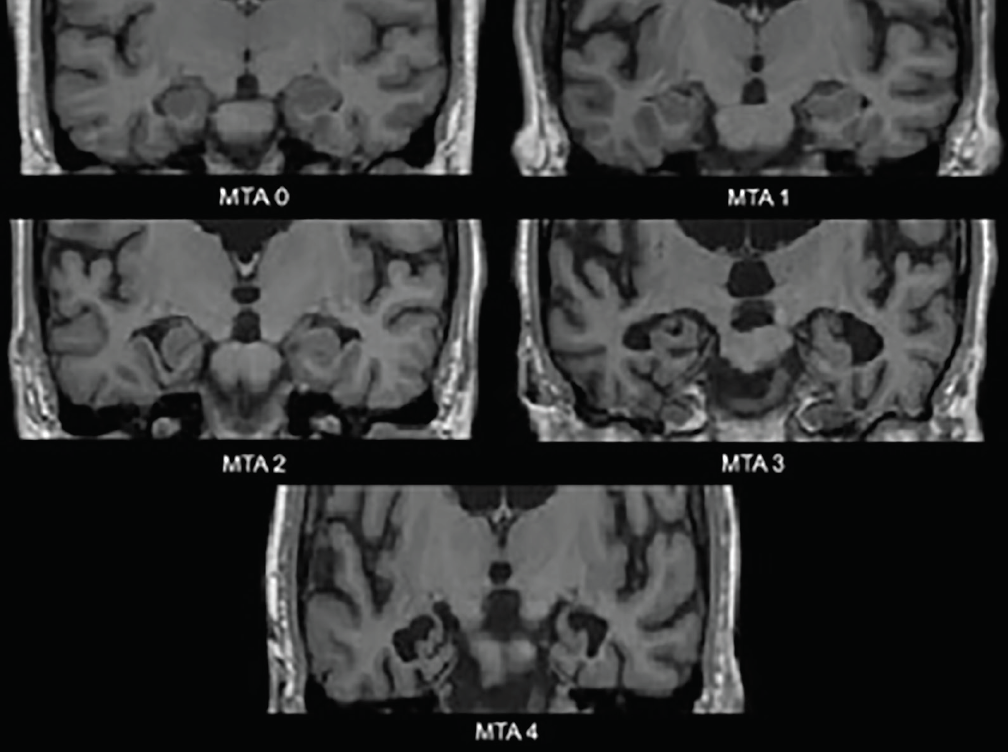
MTA score: 0: no CSF is visible around the hippocampus (normal); 1: choroid fissure is slightly widened; 2: moderate widening of the choroid fissure, mild enlargement of the temporal horn and mild loss of hippocampal height; 3: marked widening of the choroid fissure, moderate enlargement of the temporal horn, and moderate loss of hippocampal hei.

Radiologists find their voice in a patientcentric era
To assess inter-modality agreement and accuracy for medial temporal lobe atrophy (MTA) ratings across radiologists with varying clinical experience in a non-demented population. Methods Four raters (two junior radiologists and two senior neuroradiologists) rated MTA on CT and MRI scans using Scheltens' MTA scale.
Registered Radiologist Assistant ARRT
MTA-scale for Medial Temporal lobe Atrophy Fazekas scale for WM lesions Normal ageing Strategic infarctions Koedam score for Parietal Atrophy FDG-PET Specific Diseases Alzheimers Disease Presenile AD Mild Cognitive Impairment (MCI) Vascular Dementia (VaD) Strategic infarcts and small vessel disease Cerebral Amyloid Angiopathy (CAA)

Radiology Assistants and Radiology Physician Assistants Collaborative Imaging
Welcome to the Radiology Assistant. Educational site of the Radiological Society. of the Netherlands. by Frank and Robin Smithuis. Radiology Assistant is a sponsor of Medical Action Myanmar. Horner syndrome. new. Cervical Cancer - MR staging. new.

Radiologist and Assistant in the Control Room of Computed Tomography at Hospital Stock Photo
Objective To provide age-specific medial temporal lobe atrophy (MTA) cut-off scores for routine clinical practice as marker for Alzheimer's disease (AD). Methods Patients with AD (n = 832, mean age 81.8 years) were compared with patients with subjective cognitive impairment (n = 333, mean age 71.8 years) in a large single-centre memory clinic. Mean of right and left MTA scores was determined.

Medial temporal atrophy (MTA) scoring illustrated on T1weighted MRI.... Download Scientific
Visual rating of medial temporal lobe atrophy (MTA) is often performed in conjunction with dementia workup. Most prior studies involved patients with known or probable Alzheimer's disease (AD). This study investigated the validity and reliability of MTA in a memory clinic population. MTA was rated in 752 MRI examinations, of which 105 were performed in cognitively healthy participants (CH.

Radiologist Assistant (RA) Registered Radiologist Assistant The Radiologic Technologist
MTA correlation with quantitative volumetric methods ranged from -0.20 (p< 0.05) to -0.68 (p < 0.001) depending on the quantitative method used. Both MTA and FreeSurfer are able to distinguish dementia subgroups from CH. Suggested age-dependent MTA thresholds are 1 for the age group below 75 years and 1.5 for the age group 75 years and older.

Radiographs of case 1. (a) The first visit during working length... Download Scientific Diagram
Usage An ERICA score of 2 or 3 (see below) has been shown to have higher diagnostic accuracy for distinguishing healthy controls with subjective cognitive decline from individuals with Alzheimer disease than the older medial temporal lobe atrophy (MTA) score 1 . diagnostic accuracy = 91% sensitivity = 83% specificity = 98% Imaging

Image
A general problem with the MTA score is the inconsist-ently dened cuto value. Various cutos for pathological MTA scores can be found in the literature, diering by age groups and education level. For example, Velickaite and colleagues [8] elaborated that "at age 75, gender and edu-cation are confounders for MTA grading. A score of ≥ 2 is
The Radiology Assistant Dementia Role of MRI
The MTA score is a visual score performed on MRI of the brain using coronal T1 weighted images in a plane parallel to the brainstem axis and through the hippocampus at the level of the anterior pons 5. The score is also validated for assessment on CT brain 6.

MTA in Front of MRI Machine in Radiology Stock Image Image of people, machine 33010943
Medial temporal lobe atrophy (MTA) is considered as a biomarker for Alzheimer's disease (AD) [ 1 - 6] and visual MTA ratings are available for clinical use [ 7 ]. There is debate as to what cut-off scores should be used in clinical practice to optimally differentiate AD from controls without dementia [ 8] or with other types of dementia [ 9, 10 ].

The Radiology Assistant Brain Dementia Role of MRI
Results. Patients with AD had higher MTA scores (mean, 2.13) and ERICA scores (mean, 2.05) than patients with SCD (P < .001).An ERICA score of 2 or greater achieved a higher diagnostic accuracy (91%) than the MTA score (74%), with a sensitivity of 83% versus 57% and a specificity of 98% versus 92% in discriminating dementia caused by AD from SCD (P < .001).

Radiography Exam New England School of Dental Assisting
Abstract. Background: Medial temporal lobe atrophy (MTA) is a sensitive radiologic marker for Alzheimer disease (AD) and associated with cognitive impairment. The value of MTA in the oldest old (>85 years old) is largely unknown.

The medial temporal atrophy (MTA) visual rating scale. (ad) Coronal... Download Scientific
The Radiology Assistant : Epilepsy - Role of MRI Epilepsy - Role of MRI Laurens De Cocker, Felice D'Arco and Philippe Demaerel and Robin Smithuis Publicationdate 2012-09-01 In many patients with epilepsy antiepileptic drug treatment is unable to control the seizures.
Imagistica cerebrală în diagnosticul diferențial al demenței Savage Rose
Scores of MTA correlated to age and Mini-mental state examination score. When used to detect DAT from NC, the MTA showed highest diagnostic value than other scales, and when the cutoff score of 1.5 of MTA scale, it obtained an optimal sensitivity (84.5%) and specificity (79.1%) respectively, with a 15.5% of false negative rate.

Team Doctors Mta Radiology Hospital Stock Photo 148769429 Shutterstock
The MTA score, published by Scheltens and colleagues in 1992 [ 4 ], is a simple measure by which mesiotemporal atrophy can be quantified. Using the width of the choroidal fissure, temporal horn, and height of the hippocampal formation, atrophy is evaluated in five grades (0-4).